Arkansas Debates Nonprofit Health Care Subsidies and Unfair Competition
Hospitals, both nonprofit and for profit, participate in what must be a tangled and sometimes indecipherable system of government subsidies, all of which are regulated by statutes and regulations more convoluted than the most difficult tax statutes or regulations. The subsidies are apparently designed to make health care accessible to all without fundamentally altering the capitalist, profit-seeking mechanisms through which health care is allocated in the United States. Which is to say, that the subsidies are, on paper at least, calibrated so that they benefit patients who would not be part of a paying customer base anyway. By limiting the subsidies to non-customers – people who would otherwise just do without – the subsidies don’t drive capitalist health care providers out of business. Theoretically, for-profit providers suffer no loss of patronage because the people subsidized are too poor or under-insured to patronize for-profit providers in any event.
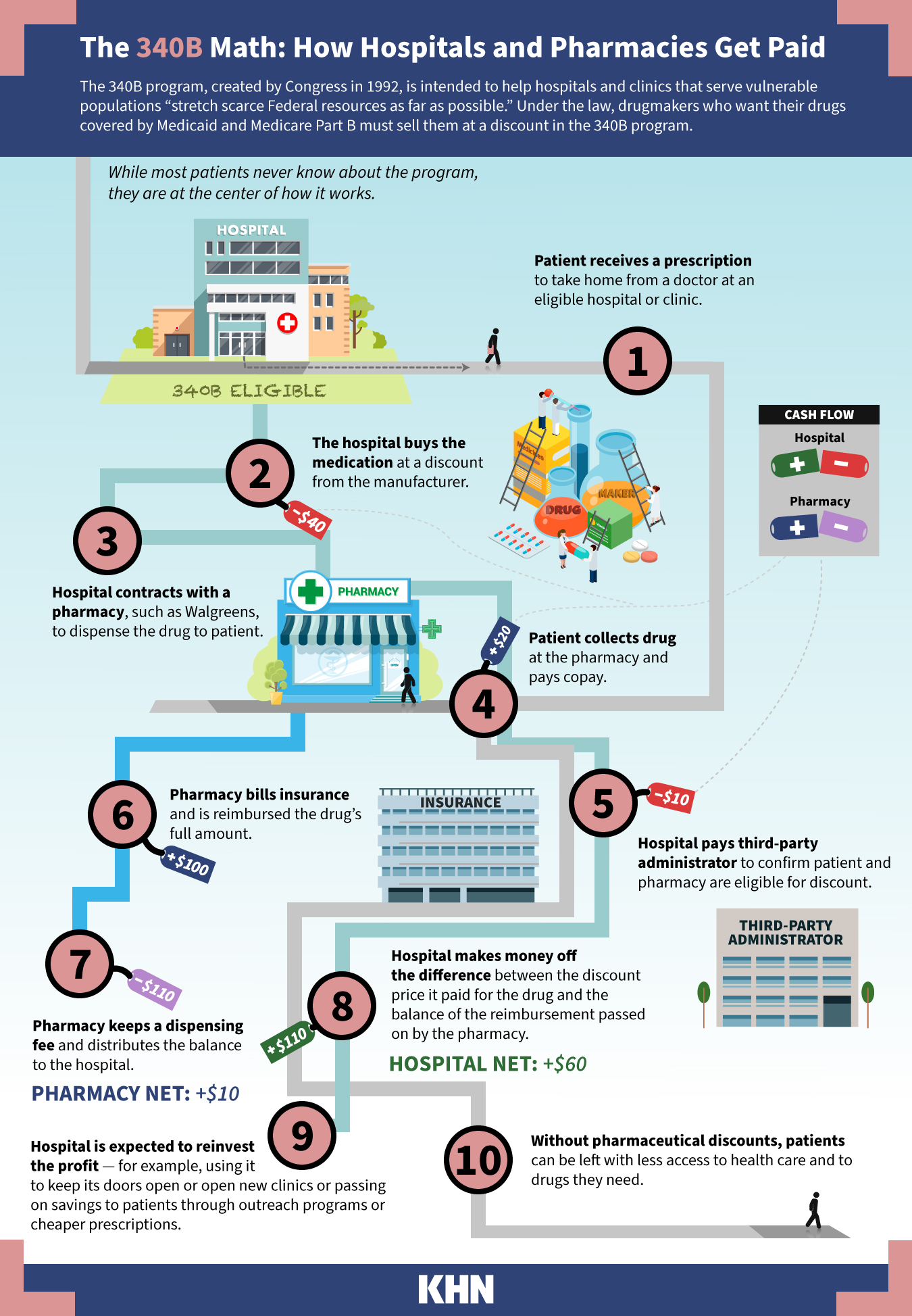
Tax exemption and the “340B drug discount program” are two examples of subsidies. Trust me, the 340B program is much more complicated than IRC 501(c)(3) is for health care. But both programs are typically geared towards charitable hospitals, though tax exemption is not required for participation in the 340B program. I know next to nothing about the 340B program, but it allows “safety net hospitals” most of which are in fact tax exempt, to acquire drugs at up to a 99.9% discount. Sometimes for one penny, even. I will assume that all safety net hospitals are nonprofit and tax exempt just for the purpose of this post.
Safety net hospitals don’t necessarily pass the discounts to their patients because they are required to sell the drugs are normal rates. In that regard, it is not apparent how safety net hospitals undercut private pharmacies by their operation of retail pharmacies except by their ability to exceed volume sold through private pharmacies. The only other instance in which safety net hospitals have an advantage is when they provide the discounted drugs for free to indigent patients who would not otherwise patronize private pharmacies anyway.
Despite the apparent “unfair competition,” or lack thereof, every state except Arkansas allows nonprofit hospitals to operate inpatient and outpatient retail pharmacies subsidized by tax exemption and the generous 340B program. By the way, nonprofit hospitals can and must sell those discounted drugs at normal [usually Medicaid or Medicare] rates and use the profit to subsidize their other charity care obligations.
In Arkansas, nonprofit hospitals are barred from operating retail pharmacies precisely because of the fear that nonprofit hospital pharmacies will drive rural privately owned pharmacies out of business. The nonprofit hospitals counter by asserting that their pharmacies increase access and outcomes for indigent patients – especially with regard to very expensive drugs that private pharmacies would not carry anyway — without negative impact on private pharmacies. Therefore, nonprofit hospitals should be allowed to operate retail pharmacies. It is the classic charity vs. unfair competition conundrum.
Last week, Arkansas’ Senate Public Health, Welfare and Labor Committee defeated a bill that would have repealed Arkansas’s law prohibiting nonprofit hospitals from operating retail pharmacies. This, despite testimony from witnesses before the vote that nonprofit hospitals would not operate in such a manner as to drive private pharmacies out of business. The nonprofits emphasized, though without much detail, that nonprofit hospitals operate retail pharmacies in every other state without the negative consequences feared by private pharmacies in Arkansas. The Committee was not convinced and voted the measure down.
I can’t speculate on which side is right or wrong in Arkansas. For some interesting background on prior failed legislative efforts, see this report from the Arkadelphian. The 90 minute hearing before the vote included interesting testimony from both sides regarding the extent to which sincere and subsidized charitable efforts nevertheless generate unintended negative consequences through unfair competition. I have often discounted the “unfair competition” rationale underlying the unrelated business income tax. But the Arkansas experience proves that unfair competition is still a legitimate concern under certain unique circumstances. The Bill and last week’s hearing exemplifies an actual contextualized debate and makes for an interesting teaching exhibit regarding unfair competition.
Yesterday, the Committee reached a compromise, passing a bill that allows nonprofit hospitals to operate outpatient retail pharmacies so long as the pharmacies are not more than 250 yards from the hospital facility. Apparently, that geographical limitation assures private pharmacies that nonprofit hospitals will not extend their reach into all corners of Arkansas.
darryll k. jones